Anatomical considerations and upper limb block
Brian D O’Donnell
Introduction
Ultrasound guidance has enabled visualisation of neural structures thereby facilitating precise, reliable upper limb blockade. UGRA is now a viable alternative to general anaesthesia on a worldwide basis. Central to the practice of UGRA is a thorough knowledge of relevant clinical anatomy. As significant inter-individual anatomical variation exists, ultrasonography permits real-time examination of clinical anatomy. The modern anaesthetist is now armed with a powerful tool to provide bespoke, individualised regional anaesthesia.
In my talk, I will concentrate on some of the common variations encountered on examination of the brachial plexus at the level of the interscalene groove, the supraclavicular fossa and the axilla. Interpretation (or misinterpretation) of the image obtained may significantly influence block outcome. The talk will also include nerves of the forearm, which exhibit the least variability in terms of location and immediate anatomical relations.
Interscalene Groove
The brachial plexus is formed by the C5-T1 nerve roots, which exit their respective intervertebral foramina, and enter the posterior triangle of the neck between the anterior and middle scalene muscles. Here they form the trunks: Upper (C5&6); Middle (C7); and Lower (C8&T1). Invested in a layer of pre-vertebral fascia, the brachial plexus travels in close and variable relation to the anterior and middle scalene muscles toward the supraclavicular fossa.
When imaged at the level of the C7 transverse process, a number of patterns of neural layout can be identified. Figure 1 summarises three of the common variations seen.
A: The superior, middle and inferior trunks are all visualised within the groove and lie within close relation to each other;
B: One of the trunks (usually the superior trunk), has a variable intramuscular course, usually within the scalenus anterior muscle.
C: The inferior trunk lies deep to the scalenus anterior muscle.
Interscalene block is useful for anaesthesia and analgesia for shoulder and proximal humerus surgery. The spatial arrangement of the brachial plexus trunks may significantly influence local anaesthetic spread and block success.
Supraclavicular Fossa
Supraclavicular block is useful for hand, forearm and elbow surgery. At the level of the supraclavicular fossa, the brachial plexus trunks have divided into anterior and posterior divisions, and given the dorsal scapular nerve, suprascapular nerve and nerve to subclavius. The plexus lies in close relation to the subclavian artery, first rib and pleura (Figure 2 A). At this level the descending scapular artery arises from the subclavian artery. This artery may be very prominent in athletes and manual workers. When visualised, it appears divide the supraclavicular plexus into two compartments (Figure 2B). Spread of local anaesthetic injectate may be limited by this phenomenon, illustrating the need to identify each of the components of the plexus and the immediate relations.
Axilla
Axillary brachial plexus block is useful for forearm, wrist and hand surgery. The terminal nerves of the brachial plexus (Median Nerve-Lateral & Medial Cords; Ulnar Nerve-Medial Cord; Radial Nerve- Posterior Cord; Musculocutaneous Nerve- Lateral Cord) lie in close relation to each other and the axillary vasculature. The arrangement of the nerves of the axillary brachial plexus around the axillary artery exhibits very significant inter-individual variability. Figure 3 illustrates many of the common variations encountered during axillary block.
A: This may be thought of as the standard arrangement of nerves, vessels and surrounding musculature;
B: The musculocutaneous nerve may lie in close relation to the median nerve (lateral cord);
C: The axillary vein may surround the neural contents, pushing them clockwise around the axillary artery;
D: There may be a duplex arterial system in the axilla (6-8%) with resultant alterations in nerve layout.
These represent the principal variations commonly encountered in my clinical practice.
Forearm Nerves (Figure 4)
Peripheral nerve block at the level of the forearm is a useful adjunct to plexus blockade. The nerves of the forearm have relatively consistent relations at fixed points. At the level of the antecubital fossa, the median nerve can be visualised as a honeycomb structure medial to the brachial artery (Figure 4A). The radial nerve at this same level has divided into a superficial branch and a deep (posterior interosseous) branch. It can be seen like a pair of eyes looking out between the brachioradialis and brachialis muscles (Figure 4B). The ulnar nerve is found in the medial forearm, between the flexor digitorum superficialis and profundus muscles, in close relation to the ulnar artery (Figure 4C).
Forearm techniques can be used as the ‘rescue’ block for failed or insufficient plexus block. It can also be used to deposit long acting local anaesthetic for post-operative analgesia when rapid return proximal limb function is desirable (e.g. axillary block for palmar fasciectomy using lidocaine, bupivacaine deposited at the ulnar nerve in the forearm for post-operative analgesia). Finally hand surgery to discrete areas not requiring an arm tourniquet (K-wire 5th metacarpal) may be performed entirely using a forearm single nerve block (ulnar nerve).
Summary
Clinician acceptance that the ‘TEXTBOOK’ description of anatomy does not necessarily exist, will permit appropriate interpretation of the ultrasound image acquired during UGRA. Correct image interpretation improves the likelihood of successful block outcome. Ultrasonography permits the identification of all anatomical types, enabling individualised, safe and effective peripheral nerve block.
Figure 1

Figure 2
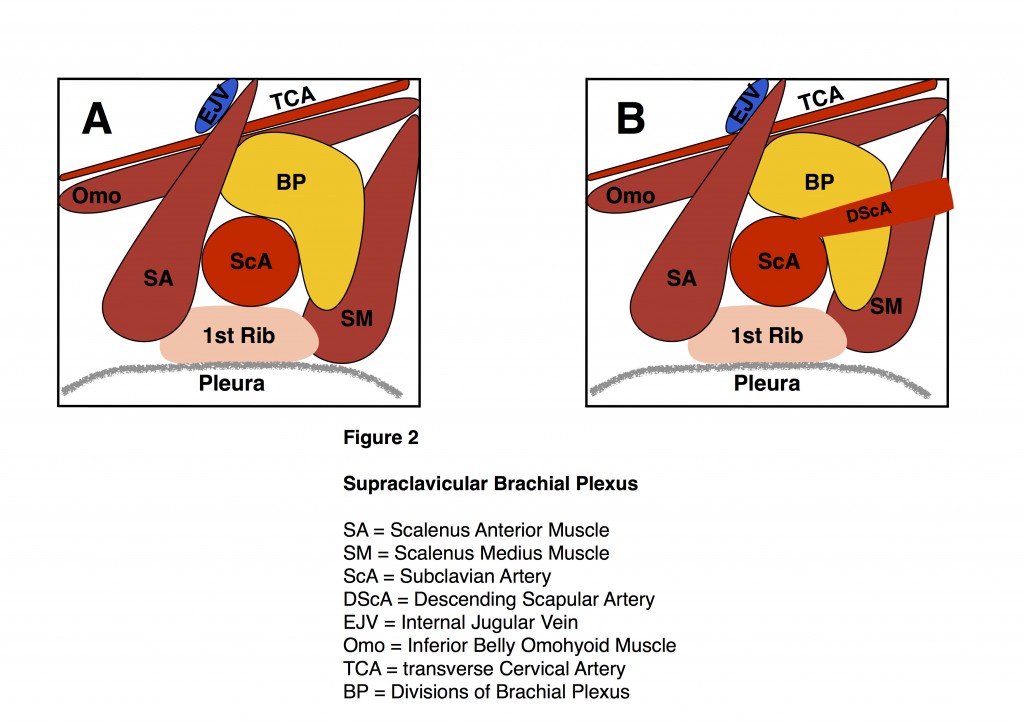
Figure 3
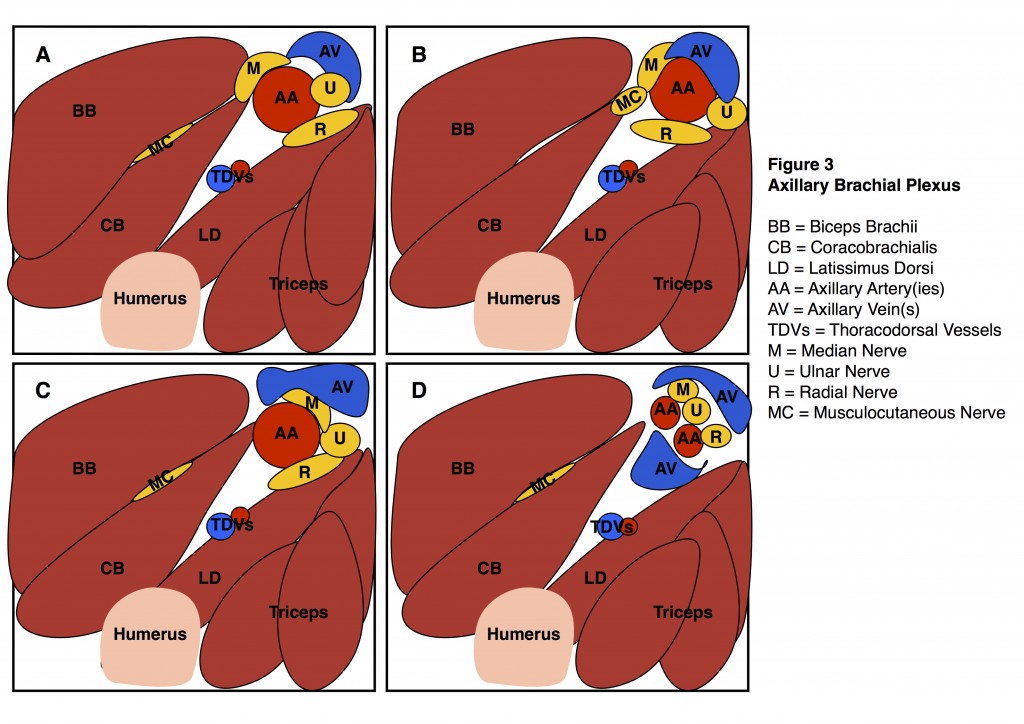
Figure 4


